Secondary hypertension
-
Most people with hypertension have primary or essential hypertension where there is no identifiable cause for their high blood pressure. However, 5 - 10% of adults with hypertension have secondary hypertension where there is an underlying and potentially correctable cause of their high blood pressure.
-
Secondary hypertension should be considered at the outset of confirmed hypertension, particularly if young without risk factors or a family history of hypertension. Secondary hypertension should also be considered if persistent hypertension despite adherence to ≥ 3 blood pressure lowering therapies
-
Causes of secondary hypertension include:
-
Obstructive sleep apnoea
-
Renovascular disease and renal parenchymal disease
-
Medications e.g. oral contraceptive pill, NSAIDs, steroids, cyclosporin etc.
-
Recreational drug use e.g. amphetamine, cocaine, excess alcohol intake
-
Endocrine disorders e.g. primary hyperaldosteronism, Cushing’s disease, phaeochromocytoma, thyroid disease and acromegaly
-
Pregnancy
-
Coarctation of the aorta
-
History and examination often provide guide to which investigations should be performed to confirm or exclude causes of secondary hypertension.
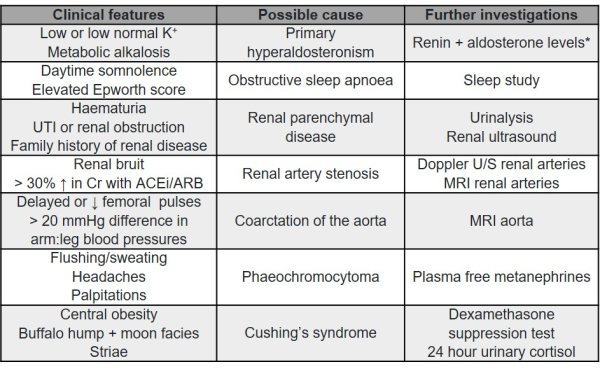
* Primary hyperaldosteronism is a common cause of secondary hypertension in adults and the aldosterone:renin ratio is best performed before starting BP lowering medications.
Choice of agent in each of BP lowering medications
The likely preferred agents in each of blood pressure lowering medications based on efficacy, tolerance and availability in Aotearoa NZ are:
-
ACEi and ARB:
-
Ramipril typically preferred ACEi but perindopril useful alternative. Quinapril also useful alternative if combination with TD desirable but often requires twice daily dosing.
-
Usual dose range of ramipril is 2.5 mg – 10 mg daily but may start 1.25 mg daily if elderly and/or risk of hypotension
-
Usual dose range of perindopril is 2 mg - 8 mg daily
-
Usual dose range of quinapril is 2.5 mg – 20 mg once or twice daily.
-
Combination with hydrochlorothiazide available at 10 mg and 20 mg doses of quinapril.
-
Candesartan typically preferred ARB
-
Usual dose range of candesartan is 8 mg – 32 mg daily but may start at 4 mg daily if elderly and/or risk of hypotension
-
Usual dose range of losartan is 50 mg – 100 mg daily but may start at 12.5 mg - 25 mg daily if elderly and/or risk of hypotension.
-
Combination with hydrochlorothiazide available at 16 and 32 mg doses of candesartan and 50 mg dose of losartan
-
CCB:
-
Amlodipine and felodipine preferred with usual dose range for both 2.5 mg – 5 mg daily
-
10 mg daily doses are associated with greater risk of adverse effects for often little additional benefit
-
Useful if elevated diastolic BP due to vasodilatory effect
-
TD:
-
Usual dose of chlorthalidone: is 12.5 mg – 25 mg daily and usual dose of bendroflumethazide is 2.5 mg - 5 mg daily. Higher doses typically lead to little additional BP lowering but greatly increase adverse effects.
-
Chlorthalidone has a significantly longer half-life (lasting up to 72 hours) compared to other TDs. This may be helpful and more efficacious, but the prolonged duration of action also means a sustained effect on renal sodium and water excretion, and should be balanced against the increased likelihood of cumulative electrolyte disturbances over time.
-
Hydrochlorothiazide is a weak BP lowering agent but may be useful if combination tablets preferable
-
β-blockers:
-
Metoprolol controlled release (CR) or bisoprolol preferred for ischaemic heart disease and rate control
-
Carvedilol likely preferable if congestive heart failure
