Choice of lipid lowering therapy
-
First line lipid lowering medications are atorvastatin and rosuvastatin.
-
Rosuvastatin is typically preferred if previous CV event but mismatch with special authority criteria
- Current special authority requires previous failures of atorvastatin or simvastatin to reach LDLc target unless Māori or Pacific ethnicity
- Maximise rosuvastatin use in Māori and Pacific peoples given funded and their high CV risk
- Other ethnicities may choose to self-fund rosuvastatin without trialling atorvastatin as cost is currently around $12 per week
-
Rosuvastatin is typically preferred if previous CV event but mismatch with special authority criteria
-
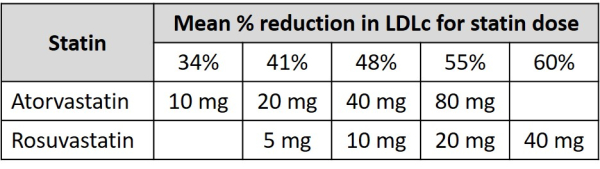
Usual dose range is atorvastatin is 10 – 80 mg daily and rosuvastatin 5 – 40 mg daily
- Consider starting rosuvastatin 5 mg daily if South East Asian ancestry due to a common genetic polymorphism that increases rosuvastatin levels
- Maximum dose of rosuvastatin is 10 mg daily if eGFR < 30 mL/min
- At least 40 mg atorvastatin or 10 mg rosuvastatin daily is typically required to achieve a 50% reduction in LDLc
-
Statins have low and potentially no teratogenicity - so statins can be used in women of child-bearing age without fear.
- Current advice is to stop statins in pregnancy and breastfeeding, but discuss with secondary care if known cardiovascular disease and/or familial hypercholesterolaemia as it may be safest to continue statin.
-
Measure non-fasting LDLc at least 3 monthly and titrate statin to reach LDLc target or maximal tolerated dose
- 90% of LDLc lowering evident within 2 weeks so do not need to wait 3 months before titrating
- Repeat testing may be barrier to optimising treatment so consider starting statin at or rapidly titrating statin to estimated dose to reach LDLc target
-
Switch atorvastatin to rosuvastatin if LDLc is above target on 80 mg daily or maximal tolerated dose
- Consider trialling pravastatin if intolerant of low dose atorvastatin and rosuvastatin
-
Consider ezetimibe 10 mg daily if LDLc above target despite maximal tolerated dose of statin
- Ezetimibe no longer requires special authority approval
- Consider evolocumab (Repatha) or inclisiran if LDLc still above target but require SC injection (2-4 weekly or 6 monthly), are not funded and are expensive (particularly evolocumab). They will reduce LDL on average by a further 50% from baseline.
- Measure non-fasting LDLc 6 - 12 monthly once treatment optimised to ensure targets are still met.
